Bimonthly assessment November
- Get link
- X
- Other Apps
Case 4
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.

CASE1:
55 year old male patient came with the complaints of
Chest pain since 3 days
Abdominal distension since 3 days
Abdominal pain since 3 days and decreased urine output since 3days and not passed stools since 3days
1.Anatomical locations and etiological possibilities:
A.Pancreas:acute severe pancreatitis secondary to gall stones
B.Kidney:Acute kidney injury secondary to pancreatitis
C.lungs:Right pleural effusion secondary to acute severe pancreatitis
Pleuropulmonary abnormalities are commonly associated with pancreatitis, respiratory dysfunction is rarely seen at the time of presentation to Emergency department (ED) but usually develops after fluid resuscitation. It manifests as acute lung injury or acute respiratory distress syndrome. It is one of the major components of multiple organ system dysfunction syndromes. Other manifestations are bilateral infiltrates, pleural effusion, pulmonary hypertension, and decreased thoracic compliance
https://www.intechopen.com/books/intensive-care/severe-acute-pancreatitis-and-its-management
D.Tibia:diaphyseal dysplasia
E.Right upper limb:atherosclerotic vascular disease
due to hypertriglyceridemia
During the first 1-2 wk, a pro-inflammatory response occurs, which results in systemic inflammatory response syndrome (SIRS), a sterile response in which sepsis or infection rarely occurs. If the SIRS is severe, then proinflammatory mediators can cause early multiple (respiratory, cardiovascular, renal, and hepatic) organ failure
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4194569/
Sequence of events
A.diaphyseal dysplasia of both tibia
B.patient is a alcoholic and smoker since 30years
C.patient has an atherosclerotic vascular disease of right upper limb
D.patient presented with chest pain,sob, decreased urine output(due to AKI secondary to sepsis),constipation(due to paralytic ileus),abdominal distension
He was diagnosed with acute severe pancreatitis(supported by clinical,USG findings and raised serum amylase levels) secondary to gall stones with AKI ,rt pleural effusion
E.patient was started on inj.lasix and iv antibiotics,after 1day pedal edema and sob decreased.after one moreday patient was in altered sensorium,on the same day patient was taken for hemodialysis 1st session.after hemodialysis his urea and creat values have come down(7.4 to 5.3)and sensorium improved.
F.After 2days patient was taken for one more session of dialysis (his creat 5.9 to 4.4) but his total leukocyte counts have been raised ?Central line sepsis.
G.within 24hrs of 2nd session of dialysis his creat increased again to 5.4 and patient had 8episodes of vomitings and was intolerant to oral feeds.
NON PHARMACOLOGICAL interventions
1.NBM:
2.Ryles tube:If nutritional support is supplemented by the enteral route, then it is usually delivered by tube feeding. There is a controversy about nasogastric versus nasojejunal feeding. But there is not much evidence to support any one over the other. Though traditionally nasojejunal feedings (to be delivered distal to the ligament of Treitz) have been preferred with the concept of less stimulation of the exocrine pancreas, cholecystokinin (CCK) cells that are present in the distal third part of the duodenum get stimulated when food passing through duodenum. It releases CCK that stimulates the pancreas and increased volume of pancreatic enzymes and bicarbonate secretion. This may worsen the course of the disease. Nasogastric tube feedings have now been shown to as safe as the jejunal feeding. Nasogastric insertion can be at bedside. Fluoroscopy endoscopic (endoscopically placed guide wire) and specialist help is not needed. With the Nasogastric (NG) feeding, the standard precautions of aspiration like elevation of head end of bed should be followed.
https://www.intechopen.com/books/intensive-care/severe-acute-pancreatitis-and-its-management
3:Oxygen support:Patients with acute severe pancreatitis should be monitored closely for early detection of failure. Respiratory support usually initiated by supplemental oxygen and mechanical ventilation is often required depending on the severity of respiratory dysfunction. Nasogastric decompression will decrease the distension and improve the compliance and prevent aspiration. Non-invasive ventilation is poorly tolerated in most of the patients because of abdominal distension and reduced functional residual capacity, careful selection of patient is warranted. Non-invasive ventilation is good choice to start with as it may avoid endotracheal intubation. Acute lung injury and Acute respiratory distress syndrome (ARDS) secondary to acute severe pancreatitis is similar to any other condition using lung protective strategies. Pleural effusion may need ultrasound-guided drainage. Good analgesia will help in chest physiotherapy, early physiotherapy will prevent atelectasis and related complications
PHARMACOLOGICAL interventions
1.Iv fluids:Hypotension is one of the most common presentations with acute pancreatitis. It is a sign of impending organ dysfunction. The hypotension is due to the third space loss secondary to the inflammatory response, this contributes to hypoperfusion and end organ perfusion dysfunction. Aggressive fluid resuscitation and rapid restoration of intravascular volume are the main stay of the treatment. It requires several liters of fluids. Both crystalloids and colloids can be used as resuscitation fluids
https://www.intechopen.com/books/intensive-care/severe-acute-pancreatitis-and-its-management
2.Diuretics:for decreased urine output and renal failure
3.Antibiotics:
Role of antibiotic prophylaxis in severe acute pancreatitis
Prophylactic antibiotics in severe acute pancreatitis have been a topic of debate in the last 4–5 decades. Pancreatic necrosis more than 30% increases the chances of infection. The right choice of antibiotics is very important, those which have high penetration into pancreatic tissue. Carbapenems are both broad spectrum and excellent pancreatic penetration properties. Other antibiotics, which penetrate well in the pancreatic tissue, are cephalosporin, ureidopenicillins, fluoroquinolones, metronidazole and imipenem. Aminoglycosides have a poor penetration ability. Patients with mild pancreatitis do not benefit from antibiotics. In a meta-analysis by Sharma et al. [16], use of prophylactic antibiotics has shown mortality benefit in patients with Acute necrotizing pancreatitis (ANP) confirmed by contrast-enhanced CT (21–12.3%). Ref. [15, 16] prophylactic antibiotics use has not shown to decrease the need for interventional and surgical management but no effect on mortality.
https://www.intechopen.com/books/intensive-care/severe-acute-pancreatitis-and-its-management
4.ANALGESIA:Pain is one of the symptoms of acute severe pancreatitis. It causes discomfort and heightened sympathetic activity, impairment of oxygenation due to restriction of abdominal wall movement. Effective analgesia can be provided by the use of opioids and parenteral route, i.e. intravenous route is the preferred route. Analgesia may improve pulmonary dysfunction. In the past, morphine was supposed to exacerbate acute pancreatitis by promoting contraction of the sphincter of Oddi and increase pressure in the sphincter of Oddi dysfunction, but there is no good supportive evidence. Another modality of pain management is use of drugs like local anaesthetics through in epidural route
https//www.intechopen.com/books/intensive-care/severe-acute-pancreatitis-and-its-management
CASE2
a) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
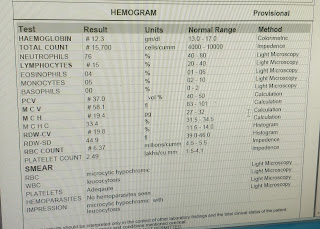
1.Pt has Anemia
2.Acute renal failure
3.lytic bony leisons ,
4.cxr and sputum reports showing pneumonia.
Anemia with low retic count
Total proteins (12.4 g/dl)
albumin (1.84 g/dl)
high gamma gap
Possible differential : Multiple myeloma
Multiple myeloma is a plasma cell dyscrasia ,where there are clone of plasma cells causing excessive production of immunoglobulins ,but these immunoglobulins are defective hence confer no immunity and these people are prone for more infections .
Multiple myeloma (MM) is a clonal plasma cell proliferative disorder characterized by the abnormal increase of monoclonal paraprotein leading to evidence of specific end-organ damage.
Anatomical locations of problems and their etiologies:

Image:archith baloor textbook of medicine pg 587
1) Bone marrow - due to marrow infiltration anemia,leucopenia,thrombocytopenia
2)lytic bone lesions pepper pot skull
3)renal failure - Excess monoclonal immunoglobulin can cause hyperviscosity, platelet dysfunction and renal tubular damage, leading respectively to neurologic derangement, bleeding, and renal failure.
excess production of monoclonal light chains (light- chain cast nephropathy), deposition of intact light chains causing nephrotic syndrome, light chain amyloidosis, hypercalcemia, hyperuricemia, dehydration.
These patients can also have bleeding manifestations due to thrombocytopenia and anitbody coated platelets which are defective.
5) Head ache ,paresthesia and blurring of vision- are features of hyper viscosity.
6) Lungs : showing Moderate to gross right pleural effusion and Multilobar consolidations of the right lung, involving upper and middle lobes With Passive collapse of basal segments of right lower lobe .
Pneumonia is because of immunodeficiency state ,as the immunoglobulins produced are defective.
Pleural fluid analysis showing exudative picture suggesting parapneumonic effusion.
SEQUENCE OF EVENTS

OUTCOMES
Median survival for newly diagnosed MM is about 44.8 months . MM cannot be cured , but new drugs are available to manage patients with MM.
https://www.hindawi.com/journals/bmri/2016/6848902/
CASE 3
5.seizures in this patient is again due to stroke .
(Infarct in right frontal lobe ).

Preload reducing agents - Diuretics (only if symptomatic)
Afterload reducing agents - vaso dilators ,ace inhibitors and arb
Beta blockers for preventing cardiac remodeling and reduce mortality.
https://pmj.bmj.com/content/79/937/634
Antiepileptics ( known case of epilepsy)
Insulin for glycemic control in diabetes.
Non pharmacological interventions
Salt and fluid restriction
https://pubmed.ncbi.nlm.nih.gov/23787719/
Individualized salt and fluid restriction can improve signs and symptoms of CHF
- Get link
- X
- Other Apps

Comments
Post a Comment